
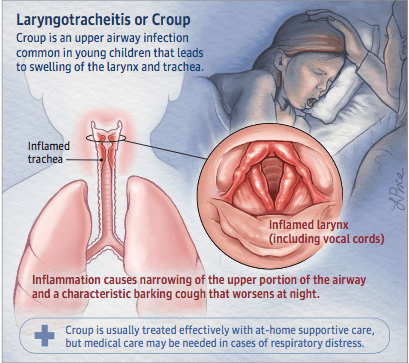
Croup is a common upper respiratory tract infection that can affect young children.
Croup typically occurs in the fall and winter months and is caused by parainfluenza or influenza viruses, adenovirus, or respiratory syncytial virus. These viruses cause inflammation of the larynx (voice box) and the trachea; hence, the clinical name of croup is laryngotracheitis. The inflammation leads to swelling and redness of these structures, which can affect a child’s voice as well as ability to breathe.
Symptoms and Diagnosis
Croup often starts, as many respiratory infections do, with a runny nose, fever, and a red, sore throat. However, within a day or two, as the inflammation progresses and the swelling worsens, a child begins to have a characteristic “croupy” cough that sounds like a seal or a barking dog. The cough is not dangerous. In more severe forms of the infection, inspiratory stridor may be heard, which is the loud sound made by the air passing through a narrowed airway when the child breathes in. Stridor is commonly accompanied by rapid, shallow, and labored breathing. The child’s nostrils flare up and the ribs can be seen with every inspiration. The diagnosis of croup is made clinically based on the symptoms and the characteristic cough. Laboratory measurements are not very useful but might show signs of infection. Testing for specific viruses with a swab can help confirm the infection but is not often necessary. An x-ray scan of the neck may help distinguish croup from other causes, but this is also rarely needed unless the initial symptoms and signs or the course of illness are different than expected.
Treatment for Croup
As with many other viral upper respiratory tract infections, treatment for croup is supportive care. Mild infections can be managed at home with over-the-counter analgesics if the child is uncomfortable. Cool or warm mist may help loosen secretions and ease breathing. As long as the child can stay hydrated, evaluation by a doctor is not necessary. However, if there are signs of respiratory distress such as inspiratory stridor or increased work of breathing, bluish color of the lips, or decreased alertness, then the child should be evaluated by a doctor or seen in the emergency department. If the stridor is severe, nebulized racemic epinephrine is used to help decrease inflammation and open the airway to allow the child to breathe. Steroids such as dexamethasone will likely be given orally, as an injection in the muscle, or intravenously. Most children improve after 1 treatment of epinephrine and steroids, while some may require hospitalization for repeat doses and hydration. Antibiotics are not useful—croup is caused by viruses. Very rarely, a child might need a breathing tube until the infection subsides.
See Also: Sick Child Pediatric Visit
Considerations
Croup is contagious in the first few days, and good hand hygiene is important. The cough may linger for weeks after the infection subsides. There are currently no vaccines available to prevent croup. Rarely, the infection can affect deeper structures such as the lower airways or the lungs (called laryngotracheobronchitis or largyngotracheobronchopneumonitis). Similarly, a bacterial infection can occur on top of the viral croup, in which case a child will be very ill and will require antibiotics and hospitalization. These more severe infections typically affect children who have underlying diseases such as asthma or who are immunocompromised.
Article courtesy of American Medical Association
Authors: Ioana Baiu, MD, MPH; Elliot Melendez,MD
Author Affiliations: Stanford Hospital, Stanford, California (Baiu); Johns Hopkins All Children’s Hospital, St Petersburg, Florida (Melendez).
Source: Malhotra A, Krilov LR. Viral croup. Pediatr Rev. 2001;22(1):5-12. doi:10.1542/ pir.22-1-5